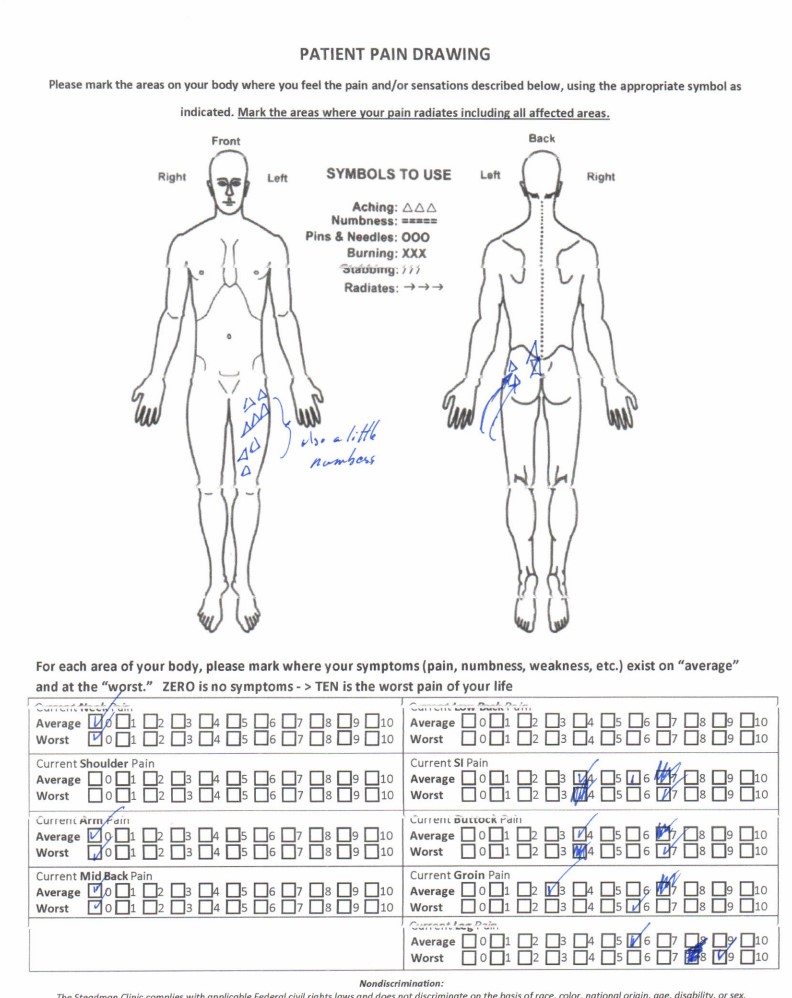
•Pain in anterior thigh with standing, walking
•Better with sitting, lying
•Awakens at night
•Stairs painful but in/out of car OK
•Has to lift his L leg by grabbing his pant leg
•Crossing legs OK
•Patient has prior L5-S1 microdisc
Physical Examination

•Reflexes and sensory intact
•Flexion full and non-painful
•Extension reproduces thigh pain
•L Psoas 4/5
•Log roll/grind “tight”
•Negative SLR test
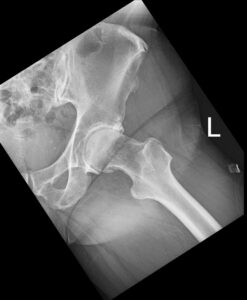
Lateral X-ray

•Significant degeneration of the L5-S1 disc
•No slips or antalgic positioning
Narrowed hip joint space with spur formation and CAM type lesion
•What signs would lead you to a hip diagnosis?
•What signs lead you away?
•Can the psoas weakness be ascribed to pain inhibition?
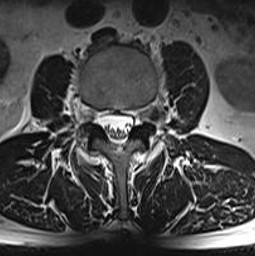
Far lateral HNP at L2-3 Left

•Typically, these far lateral HNPs cause increase symptoms with extension as the foramen becomes narrowed
•There is no reflex associated with L2 root so DTRs will be normal
•L2 services the psoas mm so weakness is neurological and not pain inhibition
L2 Radiculopathy

Anterior thigh pain most common referral for pain and paresthesias for the L2 root
Occasionally the sensory dermatome will not be diminished by a sensory exam
SLR test is normal because the L2 root is not part of the sciatic nerve. It is part of the femoral nerve (L2-4). If a femoral nerve test was performed, it would be positive
The femoral nerve test (Ely’s test) requires extension of the hip. This test could also be positive with a degenerative hip
Very rarely, paresthesias can be noted with you stretch a degenerative hip
Shorter L2 root might have better chance of motor recovery that L4-S1 roots