History

- Note significant disc degenerative changes
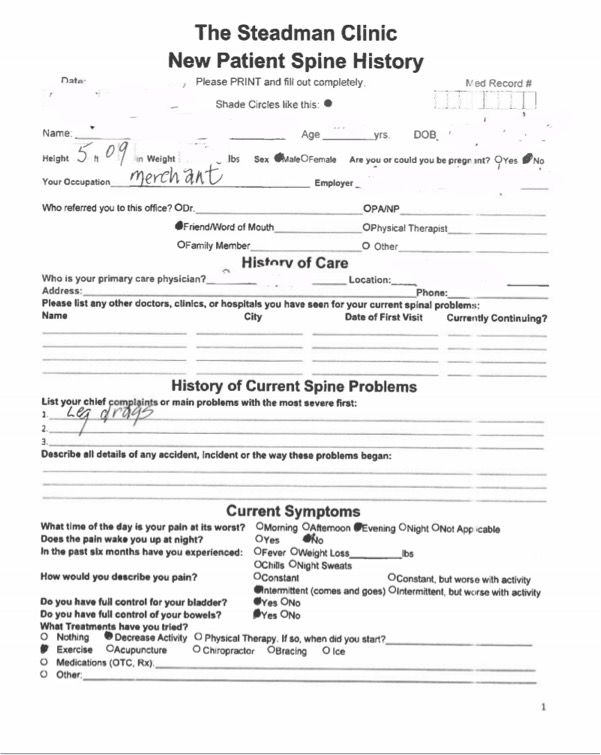
- Has LBP increasing toward EOD working in lumbar yard
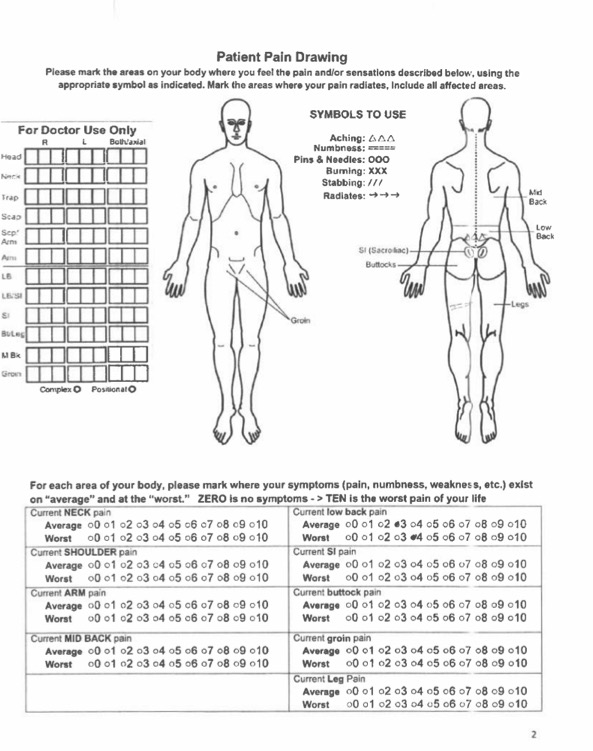
- Carefully look at pain diagram-VAS pain is 3-4
- Is that enough pain to have patient in office for degenerative disc diagnosis?
- Ask him if he would be in the office just for LBP
- Answer is no, his “leg dragging” is the real cause of his office visit
- Could this be a radiculopathy causing motor weakness without leg pain radiation?
? Radiculopathy
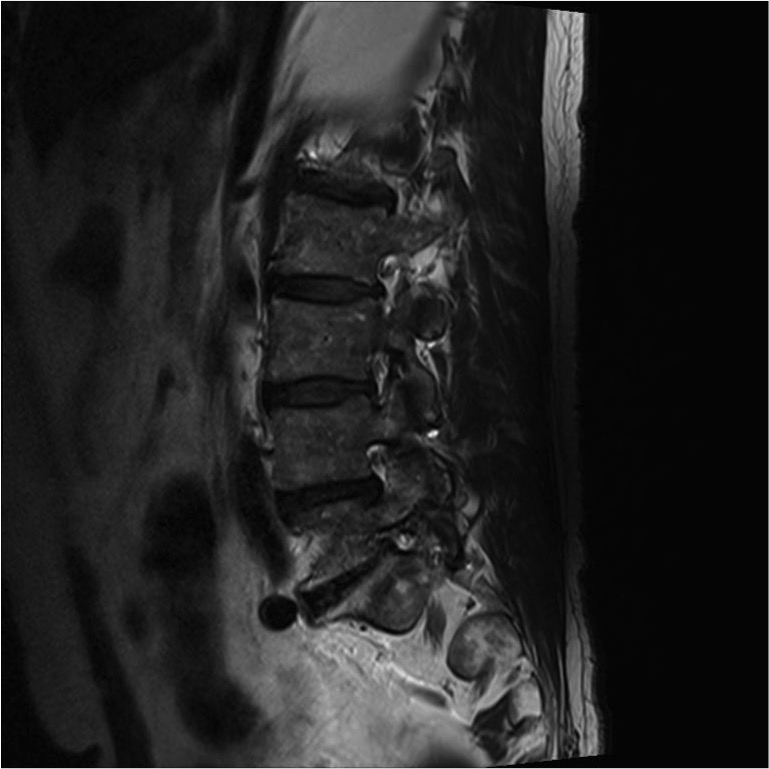
- No evidence of root compression in canal but some L5 foraminal stenosis
- Patient has no pain radiation with standing, no paresthesias, maybe occasionally catches his foot with walking (tibialis anterior weakness?)
Physical Examination
- Can heel walk bilaterally
- 5-/5 left tib anterior
- +3 reflexes bilateral lower ext and left UE
- Hoffman’s LUE
- Bilateral Clonus 3-4 beat
- After examination (thinking forward) – further careful questioning notes imbalance for last 3-4 years
- Maybe difficulty with buttons over last 5 years
- EMG/NCV neuro consult 5 years ago negative
What do you want to do next?
MRI Cervical Spine
Consider MRI thoracic spine but symptoms of loss of fine motor skills with long tract signs in LUE rule out only thoracic spine involvement
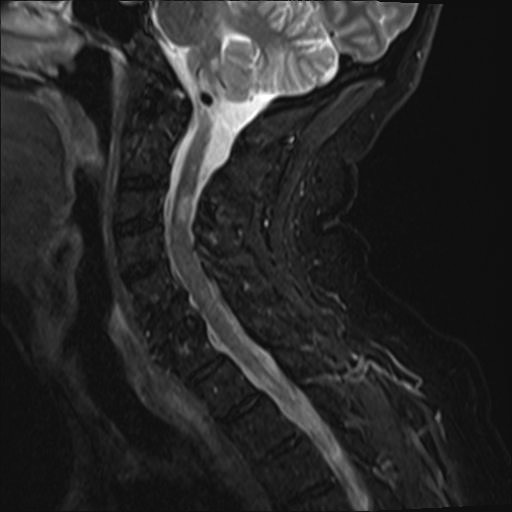
Note patchy changes in cord on STIR
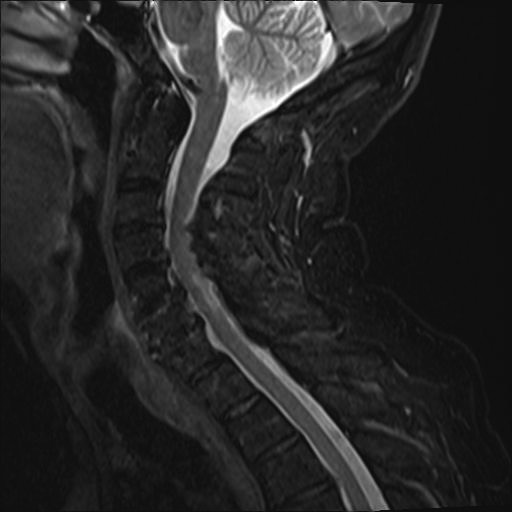
Similar changes on T2-
Dx: multiple sclerosis